Our Programs Work! Viral Suppression Rates Are250% the National Average
More than 5 in 6 have stable or improved health outcomes and over half those diagnosed with AIDS have dramatic health gains
Less than 1 in 10 HIV+ clients receive an AIDS diagnosis
Client Health Outcomes demonstrate importance of support services
Less than 1 in 10 HIV+ clients receive an AIDS diagnosis
Client Health Outcomes demonstrate importance of support services
Background
Iris House has been providing comprehensive supportive services to HIV+ minority women and their families, as well as to men and underserved populations, for 20 years through a practical, family-centered approach that promotes health while addressing the day-to-day realities of living with HIV/AIDS. These services are designed and delivered to promote and support independent functioning for our clients, to improve quality of life, and to maintain optimum health status for clients and their families. In 2013, Iris House served 387 HIV+ individuals, providing food and nutrition education, housing, case management, harm reduction services, mental health counseling, support groups and life skills training and other services in a family-centered environment by passionate, professional and culturally competent staff. In 2013 these prevention, testing and educational services and activities were provided to over 5700 community members in virtually every neighborhood in New York City as well as Plainfield and Irvington, New Jersey.
Iris House has been providing comprehensive supportive services to HIV+ minority women and their families, as well as to men and underserved populations, for 20 years through a practical, family-centered approach that promotes health while addressing the day-to-day realities of living with HIV/AIDS. These services are designed and delivered to promote and support independent functioning for our clients, to improve quality of life, and to maintain optimum health status for clients and their families. In 2013, Iris House served 387 HIV+ individuals, providing food and nutrition education, housing, case management, harm reduction services, mental health counseling, support groups and life skills training and other services in a family-centered environment by passionate, professional and culturally competent staff. In 2013 these prevention, testing and educational services and activities were provided to over 5700 community members in virtually every neighborhood in New York City as well as Plainfield and Irvington, New Jersey.
Consistent with the National HIV/AIDS Strategy and the HIV Continuum of Care,
Iris House care and case management teams focus on HIV+ client retention in care,
Viral Load and CD4 levels and changes as critical measures of client health and well-being.
|
The HIV Continuum of Care
The CDC, other federal and international agencies, local departments of health and other public and community-based agencies use what is known as the HIV Treatment Cascade. The Cascade is a visual depiction of the overall Continuum of Care for persons living with HIV (PLWH). It provides a valuable framework for thinking about the HIV service system as a whole: from diagnosis to treatment successes. Specifically, the Cascade illustrates those who are actually receiving medical care and the specific treatment needed to “make it” to the next step. The process starts with diagnoses and concludes with Viral Load (VL) suppression. A suppressed VL is the ultimate goal of the Cascade because it is consistent with improved client health and substantially lowers the risk of HIV transmission. Thus, the Cascade is a critical first step in identifying where PLWH may fall off the continuum of care and subsequently adjusting programmatic priorities. 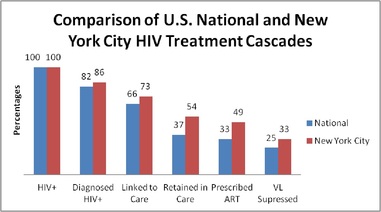
Figure 1.
|
Stages of the HIV Continuum of Care
--- Getting Tested and Diagnosed: Currently 1 in 6 in the U.S. do not know they are infected. The only way to know for sure that a person is infected with HIV is for them to take an HIV test. ---Linked to Care: Once a person is diagnosed with HIV, it is imperative that they be immediately connected to competent medical care to provide treatment which keeps them as healthy as possible and minimizes the likelihood of transmitting HIV to others. ---Staying in/Retained in Care: HIV has no cure so treatment is a lifelong process that requires a person to receive ongoing HIV medical care. ---On Antiretroviral (ARV therapy): ARV drugs are used to prevent HIV from making copies of itself and are used to control and limit the presence of HIV in the system. ---Viral Suppression: Lowering the Viral Load helps keep HIV+ persons healthy and strongly reduces the chance of transmitting HIV to others. |
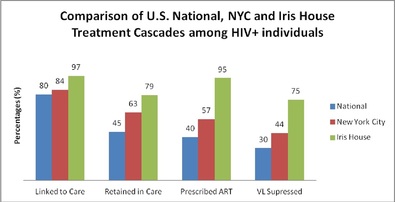
Figure 1 shows that while NYC is relatively successful along each step of the cascade, given its array of public and non-profit agencies committed to supporting those infected and affected by HIV, just slightly more than half of its HIV+ residents are on ARV and just 45% have a suppressed VL1. Nationally, less than half (45%) of HIV+ individuals are retained in care and only 3 in 10 achieve viral load suppression.
We used the city and national results in Figure 1 to measure the success of Iris House programs for its HIV+ clients. Typically, the Cascade begins with 100% estimated HIV-infection followed by the percentage that know their status. However, all of Iris House HIV+ clients are aware of their status (currently 86%) so our presentation evaluates outcomes relative to those who know their status. The agency’s data was comprised of Iris House clients who were continuously enrolled and received supportive services from January through December 2013. Figure 2 presents the cascade as above for those who have been diagnosed with HIV and know their status with Iris House in green.
Figure 2
Figure 2 shows that while most national and NYC HIV+ individuals are linked to care, virtually all (97%) Iris House clients diagnosed with HIV that receive supportive services are linked to care. Figure 2 also shows that Iris House retention and ARV rates are as high as twice the national average and well above NYC rates.
We used the city and national results in Figure 1 to measure the success of Iris House programs for its HIV+ clients. Typically, the Cascade begins with 100% estimated HIV-infection followed by the percentage that know their status. However, all of Iris House HIV+ clients are aware of their status (currently 86%) so our presentation evaluates outcomes relative to those who know their status. The agency’s data was comprised of Iris House clients who were continuously enrolled and received supportive services from January through December 2013. Figure 2 presents the cascade as above for those who have been diagnosed with HIV and know their status with Iris House in green.
Figure 2
Figure 2 shows that while most national and NYC HIV+ individuals are linked to care, virtually all (97%) Iris House clients diagnosed with HIV that receive supportive services are linked to care. Figure 2 also shows that Iris House retention and ARV rates are as high as twice the national average and well above NYC rates.
|
Iris House serves a hard to reach population, primarily women and minorities, in particular African-American, with over 90% living at or below the poverty level. For these subpopulations, as shown in Figure 3, at right, Iris House achieves VL suppression rates of 70% and 73% respectively; rates which are 250% above the national average and well above NYC rates.
The substantial improvements of the Iris House outcomes demonstrate the critical importance of supportive services that increase linkage and retention to care. Enhanced linkage/retention can improve access to medication, treatment adherence and quality of life—all critical factors in optimal health and VL suppression. They also clearly demonstrate the idiosyncratic service delivery of Iris House and its dedicated and passionate staff. VL suppression, which focuses primarily on transmission risk, is just one way to look at health outcomes. CD4 count, which helps to measure a body’s ability to fight off infection, is also used by clinicians to measure the health of HIV+ individuals. The higher the CD4 count, the better. An individual with a CD4 count of less than 200 is considered to have AIDS. Whereas a CD4 count of 500 to 1,000 is considered normal. As CD4 counts are highly variable and can change by time of day, stress, fatigue and other factors, CD4 ranges (e.g., 0 to 200, 200 to 499, 500 to 749, etc) are often used to measure changes in health. As Figure 4 shows, 86% of Iris House clients had stable or improved health as measured by CD4 and more than two-and-one-half times the number of clients saw increases in CD4 than had lower CD4 results. Further, the worse the client health when coming to Iris House, the greater the improvement after receiving services. Figure 4 classifies our clients into one of three categories: 1) individuals who came to IH with an AIDS diagnosis (CD4 < 200); 2) those who were HIV+ and with a CD4 count below normal and thus a highly compromised immune system (CD4 count between 200 and 499) and 3) those who came to Iris House with a normal CD4 level (CD4 count >= 500). For each category, Figure 5 shows the percentage that currently have CD4 counts in the AIDS diagnosis range, the below normal CD4 count range and the healthy/normal CD4 count range. |
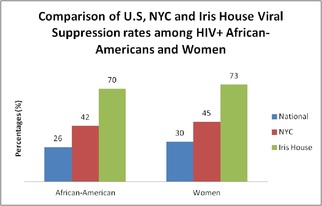
Figure 3.
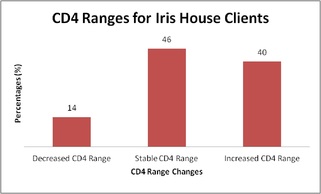
Figure 4
|
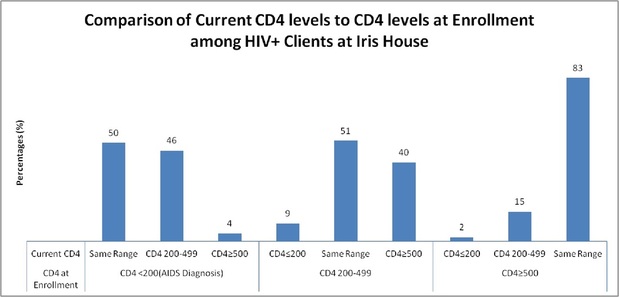
Figure 5
For those HIV+ clients who came to us with an AIDS diagnoses (a CD4 count less than 200), half now have CD4 counts over 200. Less than 1 in 10 HIV+ clients who come to Iris House and stay with us have been diagnosed with AIDS as of June 30, 2014. For those who started with below normal immune systems, over 40% improved their CD4 to a healthier, normal level. And for those who started with a normal level, over 80% stayed that way. These results are virtually identical for the women and African-American clients we serve.
Recommendations to achieve maximum Viral Load Suppression and Health Outcomes
While agencies must be responsive to the distinctive needs of their service populations, we believe that there are some lessons learned from the successes of the “Iris House Model” of combining services, resources and dedicated staff that can be incorporated by others serving an HIV+ population to enhance/maximize outcomes. In particular:
- Provide “core” services such as housing, nutrition education and meals as well as harm reduction counseling to alleviate some of the factors associated with non-adherence
- Provide care coordination/case management to ensure a holistic approach to client health that addresses related social and medical needs and enhances both treatment and medication adherence
- Provide a layer of services designed to engage and retain the client and improve quality of life, such as emotional wellness groups that increase personal accountability and responsibility, peer support, education/job and life skills training as well as transportation
- Provide a family-centered environment, which is particularly important when focusing on HIV+ women, so that mothers, grandmothers and caretakers know that they can bring their loved ones along for appointments
- Recognize that it takes a coordinated and collaborative approach to ensure clients achieve maximum health outcomes through having access to an extensive network of experienced providers internally and externally; at the same time ensuring that a client is never abandoned after a referral but is followed up with every step of the way
- Adopt a policy of “meeting the client where they are” which not only entails understanding the client’s situation and specific challenges to retention in care and treatment adherence but also includes developing individualized interventions to guide the client to improved health and optimal quality of life.
- And, most important, ensure staff understand the goals, objectives and outcomes that they are expected to achieve for the clients, identify and build upon client’s strengths and resources (both internal and external) and create a caring and compassionate environment conducive to achieving these goals.
CONTACT
For more information on this report, or the programs of Iris House, please contact Michael Smirlock, Senior Director of Administration and Performance Measurement ([email protected]) or Ursula Blanc, Director of Program Evaluation and Quality Assurance ([email protected]), by email or at 646-548-0100.
For more information on this report, or the programs of Iris House, please contact Michael Smirlock, Senior Director of Administration and Performance Measurement ([email protected]) or Ursula Blanc, Director of Program Evaluation and Quality Assurance ([email protected]), by email or at 646-548-0100.
